
I try to keep tabs on what’s new in the realm of bovine pinkeye and thought I’d share a brief update. Let’s start with where I left off in the Summer 2018 Vet Med Extension newsletter: “The reality is that there is no magic pill that can eradicate IBK. Best management practices should reduce case numbers and severity but many herds will experience IBK outbreaks periodically. In the face of an outbreak, antibiotic therapy may provide the timeliest intervention. . . . If you choose to incorporate a vaccine into management it may be prudent to isolate both Moraxella bovis and Moraxella bovoculi at the start of an outbreak to use in the development of an autogenous vaccine.”
Since then, results (Figure 1) have been published from a 5-year Randomized Control Trial (RCT) that assessed the efficacy and antibody responses to a commercial Moraxella bovis vaccine (8 strains included; Ocu-guard MB-1, Boehringer Ingelheim), an autogenous vaccine containing Moraxella bovis, Moraxella bovoculi, and Mycoplasma bovoculi (Phibro Animal Health Corporation), and a sham vaccine simply containing adjuvant. The good news is that when comparing the autogenous vs commercial vs sham vaccines there was an overall numerical difference in the cumulative incidence of IBK (24.5% vs. 30.1% vs. 30.3%, respectively, p = 0.25). Similarly, there was a numerical difference in the cases of IBK that required retreatment (21.4% vs. 27.9% vs. 34.3%, respectively, p = 0.15). Those results may have some biological importance but as you can see neither of those outcomes met the typical statistical p-value cut-off (p ≤ 0.05) to consider the differences “significant”.
An important takeaway from this research can be seen in Figure 1. First of all, note that IBK incidence data from 2016 and 2018 were omitted from the analysis because those years did not meet the epidemiological IBK case definition due to low incidence of disease. Second of all, note that IBK incidence by year ebbed and flowed such that in 2017 and 2020 the autogenous vaccine seemed to outperform the commercial and sham vaccines, yet underperformed in 2019. Similarly, the commercial vaccine appeared to be the worst option in 2017 but held its ground against the autogenous vaccine during 2019 and the sham vaccine in 2020. My point is that even though the averages suggested a numerical improvement from using the autogenous vaccine, there was no consistent pattern in terms of vaccinal benefits to overall IBK incidence. Furthermore, regardless of vaccine use there were two years during this study with a low incidence of disease. These findings fit with the historical record that suggests a complex (and irritating) dance between Moraxella bovis strain variations, incidence/prevalence, and animal or herd level resistance driven by vaccine administration or natural exposure.
A second RCT was published in 2023 (read on ScienceDirect.com) that assessed an intranasal Moraxella bovis cytotoxin vaccine. The thought behind intranasal cytotoxin vaccines is that since IBK occurs on a mucosal surface, intranasal vaccination may boost local ocular immunity. The vaccine used in this study is experimental (i.e., currently unavailable commercially), and was administered as two doses 21 days apart. The cumulative proportion of steers with ulcerated eyes at week 8 was less in the Vaccine group (25%) compared to the Control group (31%); however, this difference was not significant (p = 0.40). By week 16 (study day 112), IBK had developed in 34 steers from each group. The median healing time of the initial corneal ulcer event was 14 and 17.5 days for IBK-affected steers in the Vaccine and Control groups, respectively, but these differences were not significant (p = 0.41). The median overall cumulative corneal ulcer surface area for IBK-affected steers was 0.09 and 0.15 cm2 in the Vaccine and Control groups, respectively; however, this difference was not significant (p = 0.14). The proportions of IBK-affected steers that required treatments with oxytetracycline, flunixin meglumine, or florfenicol were all lower for steers in the Vaccine group, but the differences from the Control group were not significant (p > 0.16). And mean body weight changes between day 7 and day 112 were similar between groups. Are you starting to see a pattern emerge in terms of the limitations of pinkeye vaccines?!
That said, IBK-affected steers in the Vaccine group did have significantly more observation weeks with a low maximal corneal ulcer score (CUS 0 or 1 versus 2 or 3) compared to IBK-affected steers in the Control group (p = 0.05). Given this differences it’s worth noting that ulcerated eyes attributed to IBK were assigned a corneal ulcer score (CUS) using a previously established 4 point scoring system (Read on ScienceDirect.com) : 0 (no ulcer); 1 (maximal ulcer diameter ≤5 mm); 2 (maximal ulcer diameter >5 mm); or 3 (perforated corneal ulcer as assessed by evidence of globe rupture or visible prolapse of the iris).
Ok so what’s the take-home message? Well, the results showed that while the experimental vaccine did not reduce the incidence of IBK, it reduced ulcer severity associated with IBK. This conclusion was primarily supported by the increased number of observation weeks with a lower corneal ulcer score in the Vaccine group, but also by the findings that the median initial ulcer healing time of Vaccine group steers was 3.5 days less than the Control group, and the median cumulative ulcer area across the 16-week study period was lower in the vaccinated steers. Furthermore, the proportions of IBK-affected animals that required treatment with an antibiotic or flunixin meglumine were numerically lower in Vaccine group animals. Although these latter differences were not statistically significant, collectively they suggest that steers in the Vaccine group experienced less severe IBK compared to steers in the Control group. This is good news in that it indicates the potential for a novel vaccine strategy for reducing disease severity even if the prevention of IBK remains a complex challenge. Of course, more research is always in order and the authors of the study concluded that there is a need to determine if the vaccine used in their study offers advantages over the same antigen administered parenterally and/or if it offers advantages over existing commercially available or autogenous parenterally administered IBK vaccines.
Guess what? The lead author of the study recently presented new results at the 2026 Conference of Research Workers in Animal Diseases held January 17-20. Although the results are only in the form of an abstract and more is to follow, it’s worth noting that intranasal vaccination with adjuvated secreted Moraxella bovis and Moraxella bovoculi antigens seemed to improve some of the outcomes above. The proportion of steers that developed IBK still was not significantly different between groups. Similarly, even though the median healing time of corneal ulcers was shorter in the experimental vaccine group, the difference from control group animals was not significant. However, cumulative ulcer sizes were significantly lower in the experimental vaccine group compared with the control group, and clinical severity scores, ulcer scores, and requirements
for antibiotics were all significantly lower in the experimental vaccine group compared with the control group. The bottom line is that novel vaccine development is a work in progress but some of the leaders in the field do indeed seem to be making progress!
Given all of that, I think the summary points for consideration remain much that same as those we listed back in 2018:
- Current vaccines may not work for a specific herd because of bacterial strain differences.
- Autogenous vaccines can be made from strains isolated from the herd but there may be a different strain the following year.
- *side note* During my MS graduate studies I had the privilege of learning from one of the original pili-based vaccine researchers in this field, HG Jayappa, and he suggested that limiting the Moraxella bovis to a maximum of three strains within a vaccine may help reduce antigen dilution and improve outcomes (hence the original tri-valent vaccines). If you’d like to do a deep dive into some of the original research on pili immunogenicity you can find a publication from 1985 and a second from1986.
- Consider management such as mineral status for good immune system function of the cattle and aggressive fly control to prevent transmission.
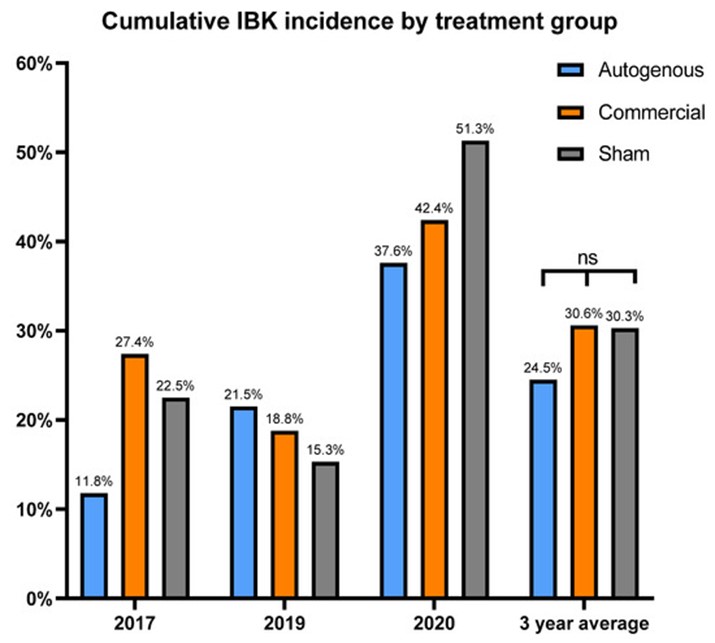
Figure 1. Annual and 3-year average incidence of IBK diagnosis by vaccine treatment group. Percentages calculated as the number of IBK diagnoses per calves enrolled each year. Vaccine treatment did not significantly affect IBK incidence. ns = not significant (p = 0.25).