By Dr. Gary Haldorson, College of Veterinary Medicine
Washington Animal Disease Diagnostic Laboratory (WADDL)
Neospora caninum was first identified as a unique pathogen in the 1980’s, having been misidentified as a new subspecies of Toxoplasma up until that time. This protozoal organism causes neurologic disease in dogs and abortions in cattle. In the 1990’s, Neospora diagnosis as the cause of abortion outbreaks within herds was commonplace. Although Neospora-induced abortion epidemics still do occur, it is much more common to see sporadic or endemic abortions within a given herd today.
Diagnosis of Neospora as the definitive cause of an abortion can be difficult. Although there are multiple tests available to diagnose infection including serology, histopathology, immunohistochemistry, and molecular diagnostics (PCR), interpretation of test results requires an understanding of the life cycle and epidemiology of the organism. Before we discuss test interpretation, we should understand what each test actually is evaluating, add in our knowledge of the organism’s life cycle, and then discuss the difficulties in diagnosis.
Diagnostic testing
Serologic testing (ELISA performed at WADDL for cattle) tests for exposure to the organism. An elevated titer requires that an animal be exposed to the organism, become infected, and mount an immune response measured by the production of antibodies specific to that organism. As with most infectious diseases, it can be difficult to equate the presence of antibodies or even the actual antibody titer to current infection versus previous exposure. In addition, even though the dam would have to be exposed and infected in order to mount a serologic titer, it does not necessarily mean that this infection was the actual cause of abortion (more on this after we discuss epidemiology).
The second test mentioned is histopathology. If a fetus is aborted due to infection with Neospora caninum, pathologists would expect to see histopathologic changes in the brain and hopefully within at least one additional tissue (such as heart). This obviously implies that the fetal tissues would have to be available for collection and submission for a bovine abortion panel. Although the lesions of Neospora can be multifocal, they tend to be numerous enough that multiple lesions will be identified even with the random nature of sections of brain, heart, and other tissues processed for histopathology. In short, if there are not enough lesions to be identified by histopathology, it is unlikely that the abortion was due to Neospora. Furthermore, it is often possible to identify protozoal tissue cysts within sections examined microscopically, and this also greatly aids in the diagnosis. However, observing the tissue cysts is less consistent than identifying the histologic foci of necrosis and inflammation that infection leaves behind.
Immunohistochemistry (IHC) was traditionally used as a confirmatory test after seeing lesions microscopically. IHC would be positive in tissues where Neospora antigens are present, and if that positive immunoreactivity was present in the foci with histologic changes, it would confirm Neospora as the cause of those changes. With the higher sensitivity of PCR, IHC has been replaced by PCR as the gold standard for diagnosis of infection. Given the expense of maintaining antibodies for IHC and the overall expense of IHC, IHC for Neospora is no longer offered at WADDL.
As mentioned, the sensitivity of PCR for diagnosis of infection makes it ideal for identifying the organism within tissues. This test can identify as few as one organism in one gram of tissue. In addition, the PCR used for Neospora at WADDL is a duplex PCR that also will detect Toxoplasma if present. Given that Toxoplasma would be the primary differential for the microscopic lesions seen with Neospora, testing for both organisms at the same time greatly enhances the test’s value, even though Toxoplasma would be a much less common cause of abortions in cattle. Still, it is actually the sensitivity of the PCR test for Neospora which further complicates its interpretation in bovine abortions (more on this after discussing the life cycle and epidemiology of infection).
Neospora caninum life-cycle and epidemiology
Dogs and coyotes (as well as dingoes and gray wolves) are the only known definitive host species for Neospora caninum. This means that only these species can be infected orally with the organism and later produce infective oocysts in their feces. Other species including rodents, rabbits, birds, cats, cattle, wild mammals, sheep, and goats, (among many other species), can serve as intermediate hosts. When exposed to the infective oocysts orally, these intermediate hosts will become infected and have the protozoa migrate systemically, ultimately forming tissues cysts filled with a life stage of the organism called bradyzoites in various tissues. However, these species will not produce infective oocysts in their feces. Instead, in these species the tissue cysts serve as a reservoir of infection that if consumed by the canine definitive host will infect the dog allowing completion of the life cycle.
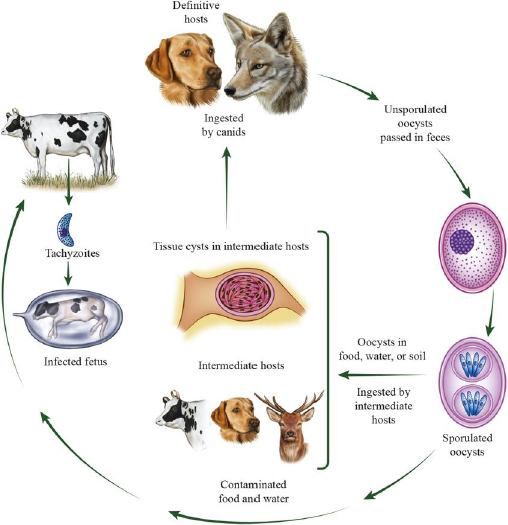
In infected cattle, there is a third life stage called the tachyzoite that can spread within the host and also cross the placenta to infect an unborn fetus. Some of these infected calves will die in utero and subsequently be aborted. (Notably, infected fetuses and placentas can serve to perpetuate the organism’s life cycle if consumed by canines). However, many cows will transmit the parasite to the fetus, but the fetus will survive (often with no clinical signs). That calf will be infected for its life and potentially transmit the parasite to its offspring. In these cases, cows that had been infected and have had parasites in their tissues in the form of tissue cysts will have recrudescence of infection at around 5 to 7 months of gestation. At that time, the parasite that was within tissue cysts in the bradyzoite phase will be released from the cyst as the more rapidly dividing tachyzoite phase and those tachyzoites will go on to infect the developing fetus. If that infection of the fetus is severe enough and causes many lesions in multiple tissues the calf will be aborted. On the other hand, if the infection is limited the calf will be infected but not aborted. It appears that this “vertical transmission” from cow to calf, in addition to contamination of feed sources with the feces from infected wild or domestic canines, serves to perpetuate infection within a given dairy herd. The mechanism of perpetuation in beef herds (infection from contaminated feed vs. vertical transmission) is less well defined. Direct infection from cow to cow (“horizontal transmission”) does not occur.
In naïve cow herds that have never been exposed to Neospora caninum, infection of feed will tend to produce “abortion storms” where several cows will abort at around the same time (shortly after the contaminated feed was consumed). Once Neospora becomes endemic within a given herd, many of the cows will become persistently infected and develop some degree of immunity. This immunity will not clear the infection in the cow and will not prevent recrudescence of infection and thus will not prevent spread of infection to the fetus. However, it does seem that the immunity is able to limit spread to the fetus and prevent abortion from occurring. This is demonstrated by the finding that primiparous heifers and cows that become infected for the first time as adults will tend to abort more commonly, whereas in subsequent pregnancies cows will most oftenproduce live and healthy (though infected) calves. Attempts to develop an effective vaccine that will either clear infection or even just reduce the likelihood of abortions occurring have thus far been unsuccessful.
Difficulties with diagnosis
Limitations of the available diagnostic tests and complexities of the life cycle of the organism result in difficulties with diagnosis of Neospora either as the cause of a given abortion or as a tool in disease management. As stated, serology is a measure of exposure and infection within the cow. Worldwide estimates of seropositivity in cows range from 15 to 40%, but within a herd infection rates can be as high as 90%. Thus, the use of serology as a potential test to identify infected cattle for the purpose of culling is troublesome. It could result in the loss of valuable genetics while not doing anything to prevent re-exposure by farm dogs or visiting coyotes. Furthermore, using serology of the cow in diagnosis of abortion is problematic at best. If seroprevalence in a herd is high, a positive titer would not be useful in confirming that the abortion was due specifically to Neospora. In addition, documenting rising titers (commonly used to differentiate preexisting infection or exposure from active infection) does not work well with this organism. As discussed above, infected cows will typically harbor an infection for life in the form of inactive tissue cysts. At 5 to 7 months of gestation, something triggers these cysts to rupture and release the tachyzoite phase of the organism’s life cycle, which will then very efficiently cross the placenta and infect the calf. This stage of gestation is correlated with an increase in antibody titers in the cow. Unfortunately, this increasing titer will occur in cows that abort due to Neospora, but also in cows that transmit the organism to what would otherwise have been a healthy (but infected) calf that was actually aborted due to a completely different cause. In effect, we expect to see a rising antibody titer in all infected cows at mid- to late gestation whether or not they abort due to Neospora.
Histopathology has a distinct advantage over serology in that the pathologist is looking at the fetal tissues for actual lesions associated with infection. Large numbers of lesions in the brain and other tissues of an aborted calf greatly increases the suspicion that Neospora was the cause, which can then be confirmed by PCR. If only one or a very few lesions are seen, then interpretation is difficult. As discussed, it is expected that a calf from an infected cow will be infected at birth and may have lesions associated with that infection. The difference between an infected calf that was aborted due to Neospora and one that was aborted due to something else is the severity (number) of lesions. This is also why we hope to see lesions in other tissues in addition to the brain in order to feel comfortable with diagnosing Neospora as the cause. While much less common as a cause of abortion in cattle, Toxoplasma gondii can result in similar lesions in the fetus, and this is why PCR is suggested in addition to histopathology to confirm the diagnosis.
PCR of fetal tissues is the current method to specifically identify Neospora as the cause when lesions are identified histologically. However, it is the sensitivity of the test that makes some interpretation of results necessary rather than just saying it is positive or negative. A negative PCR can normally be taken as an indication that Neospora is not present and thus not the cause of a given abortion. It is the calves with positive PCR results that are the problem. The PCR test is so sensitive that it can detect as few as one organism in one gram of tissue. This means that a test is expected to be positive whether a calf was aborted due to Neospora or infected but aborted due to some other cause. It is actually the combination of a positive PCR together with identification of large numbers of lesions seen histologically that results in confident interpretation of Neospora as the cause of abortion.
Summary
The diagnostics available for Neospora caninum detection require an understanding of the tests as well as an understanding of the life cycle of the parasite. Serology is an excellent test for exposure to the organism and herd infection status. It is not a good test in an individual animal to diagnose Neospora as the cause of an abortion. Histopathology is an excellent test for detecting actual lesions in an aborted fetus but has some subjectivity in interpretation by the pathologist and obviously requires the availability of fetal brain and other tissues. PCR is an extremely sensitive test for detection of infection but should not be used alone for determination that Neospora was the cause of a given abortion. The “gold standard” for diagnosis should include histopathology with appropriate lesions and confirmation of the cause with PCR. This disease is one more example of the need for good communication between the clinician and laboratory microbiologist and pathologist to appropriately interpret test results.